In April 2019, “I finished an article entitled A Woman’s Right to Safe Healthcare Outcomes.” I spent six weeks reading about this for a group which asked me to write on it from a male’s perspective. It took me all of that time. I could have doubled the size of the article I wanted to write to get the information out there. There was much to be said about the dangers women face becoming pregnant and giving birth. What prompted the resurrection of this post from 2019 was reading the efforts of SCOTUS to turn the clock back on abortions and other care. The men in black are not your local doctor or obstetrician. These are lawyers who became judges who will walk away once Roe v Wade is overturned. It is just a start of the courts interfering with
Topics:
run75441 considers the following as important: Education, Healthcare, Hot Topics, Maternal Healthcare
This could be interesting, too:
NewDealdemocrat writes JOLTS revisions from Yesterday’s Report
Joel Eissenberg writes No Invading Allies Act
Bill Haskell writes Families Struggle Paying for Child Care While Working
NewDealdemocrat writes January JOLTS report: monthly increases, but significant downward revisions to 2024
In April 2019, “I finished an article entitled A Woman’s Right to Safe Healthcare Outcomes.” I spent six weeks reading about this for a group which asked me to write on it from a male’s perspective. It took me all of that time. I could have doubled the size of the article I wanted to write to get the information out there. There was much to be said about the dangers women face becoming pregnant and giving birth.
What prompted the resurrection of this post from 2019 was reading the efforts of SCOTUS to turn the clock back on abortions and other care. The men in black are not your local doctor or obstetrician. These are lawyers who became judges who will walk away once Roe v Wade is overturned. It is just a start of the courts interfering with healthcare and especially healthcare for women.
This morning I wandered over to Crooks and Liars. Heather’s article “GOP Governor Refuses To Say If They’re Coming For Birth Control Next” discusses a conversation between Mississippi’s Head Moron Governor Tates Reeves and CNN’s Jake Tapper. Enlightening conversation reading how Reeves deliberately avoided answering the questions.
Digby at Hullabaloo also has an article up on Maternal healthcare. One graph I had used in my 2019 presentation was in that article. “The Republicans are trying to convince Americans that forcing women to bear children against their will is no big deal because they’ll be providing all kinds of services to help them go through an unwanted pregnancy and childbirth.
There is nothing to hold them to their promises of additional healthcare for women especially in the 12 states which have not expanded Medicaid. The governor of Mississippi is male and most of the legislators are male too. Their knowledge is scant except for handing out cigars. They do not care.
One thing I keep harping on. The impact of the 2016 election when people voted for communists, libertarians, Mickey Mouse, Goofy, their neighbors, etc. to avoid either trump or Clinton is coming home to roost. trump’s tour did a lot of damage to the country setting us back a decade if the men-in-black have their way. Not so funny now, yes?
As I said, I wrote this in 2019 at Angry Bear. It is still relevant.
Maternal Mortality
Healthcare for women and maternal mortality is an important indicator of a nation’s overall quality of healthcare.
Even though maternal mortality worldwide dropped 44% between 1990 and 2015; 830 women die every day from causes related to pregnancy and while giving birth. Much of it is preventable. Ninety-nine percent of all those maternal deaths occur in developing countries. WHO launched an initiative to meet the needs of those women in developing countries. The objective being to address access to and the quality of reproductive, maternal, and newborn healthcare services. Everyone would agree the effort is necessary in developing countries.
One would think the maternal rate of death in a highly developed nation such as the US would be lower when compared to developing countries and similar nations. Why not? With the advent of the PPACA, many preventative healthcare measures were put in place for women. Expanding Medicaid was possible in many states due to greater subsidies. Twelve states including Mississippi refused to expand Medicaid even though the expansion was heavily subsidized.
US citizens spend far more for healthcare to have less than or similar access to healthcare as other countries. And yet every year in the U.S, 700 to 900 women die from pregnancy, or birth-related causes. An approximate 65,000 almost die due to complications. Contrary to what healthcare should be in the US, the opposite is true. It ranks low in providing maternal healthcare when compared to the rest of the developed world.
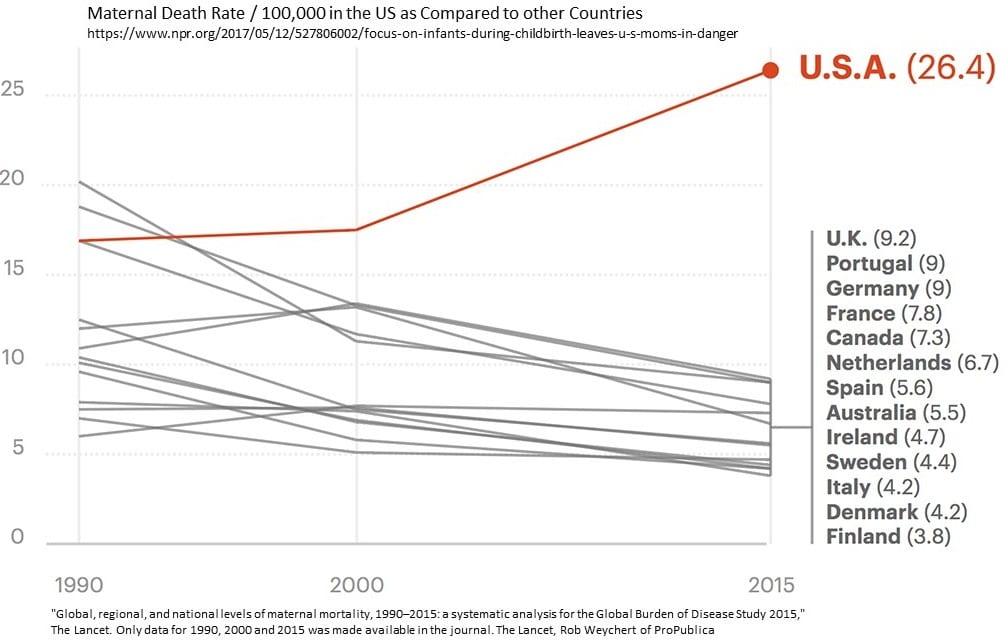
This is true even with the PPACA, expanded Medicaid in place. When compared to their Canadian sisters, American women are three times more likely to die from the start of a pregnancy up till one year after the birth of a child (defined by the Centers for Disease Control/NPR). The death rate for American women is 26.4 deaths per 100,000 as opposed to 7.3 deaths per 100,000 in Canada (Chart – click to enlarge). The ratio worsens when a comparison is made to Scandinavia countries. American women are six times as likely to die as Scandinavian women.
Two Stories to Tell
There are two stories to tell One for economically secure women and another for minority, native American, rural, and lower income women. The statistics worsens for women of color with their being more likely to die in pregnancy or childbirth and are nearly four times more likely to die from pregnancy-related causes than white women. In high-risk pregnancies, African-American women are 5.6 times more likely to die than white women. Amongst women diagnosed with pregnancy-induced hypertension (eclampsia and pre-eclampsia), African-American and Latina women were 9.9 and 7.9 times in danger of dying than white women with the same complications. Native American and Alaskan Native women experience similar discriminatory care.
Previously, half of all U.S. Medicaid births only covers women up to two months past delivery. This left a substantial gap after childbirth when other issues can arise up till a year later. As of recent, the Biden administration has extended Medicaid maternal healthcare coverage for 12 months. Medicaid left had left those who could not afford healthcare at risk.
Emphasis on Babies
Barbara Levy, vice president for health policy/advocacy at the American Congress of Obstetricians and Gynecologists;
“We worry a lot about vulnerable little babies and we don’t pay enough attention to those things catastrophic for women.”
The emphasis has been on safe baby care and safe birthing which lead to a significant decline in baby mortality. As reported in a Propublica, NPR report, the difference in “maternal mortality numbers contrast sharply with the impressive progress in saving babies’ lives.” Maternal death rates while giving birth and up to one year later has increased by an approximate 10 deaths per 100,000 since 2000 till 2015 or greater than the 9.2 deaths per 100,000 in the U.K, (Chart).
Less Emphasis on the Mother
Maternal care ignored problems occurring before, during, and after delivery. Doctor can miss a sign of a mother in stress while giving birth.
Mary D’Alton, chair of ob/gyn at Columbia University Medical Center and author of papers on disparities in care for mothers and infants.
“The training was quite variable across the U.S., there were some fellows that could finish their maternal-fetal medicine training without ever being in a labor and delivery unit. When I had my own child I realized, ‘Oh my goodness. That was completely insufficient information.’”
And doctors can fail to heed the warning signs a woman or her symptoms are alerting them too.
Elizabeth Howell, professor of obstetrics and gynecology at the Icahn School of Medicine, Mount Sinai Hospital.
“The way that we’ve been trained, we do not give women enough information for them to manage their health postpartum. The focus had always been on babies and not on mothers.”
One Mother in Stress
With 39 weeks of a good pregnancy, the expectant mother went to the hospital to induce labor. Inducing typically ends up with a cesarean delivery. Twenty-three hours later, the mother delivered normally, a healthy baby girl. The only reoccurring issue being sharp pains in the kidney area. Alleviating the pain was with more epidural. In 20 hours, a healthy mother before the birth of her daughter died after the birth.
The pain came back 90 minutes after the birth. Lauren’s doctor husband was asking questions of the ob/gyn. He was told it was acid reflux. Acid reflux is a common reaction after birthing. The pain increased; and her blood pressure spiked at 169/108. Her husband asked the OB whether this could be preeclampsia (which he suspected).
Lauren’s blood pressure upon admission was 147/99. She was experiencing similar readings during labor. For 8 hours no readings were made. All eyes were on the health of the baby, not on the mother, and what could be coming to pass. For a woman with normal blood pressure such as this young mother, a blood pressure reading of 140/90 could be indicative of preeclampsia.
Preeclampsia is a serious medical condition that can occur about midway through pregnancy (after 20 weeks). People with preeclampsia experience high blood pressure, protein in their urine, swelling, headaches and blurred vision.
Her husband reached out to another doctor. After anxiously relaying the symptoms, she quickly diagnosed what the young mother was suffering from . . . a disorder called HELLP syndrome or Hemolysis, (a breakdown of red blood cells); Elevated Liver enzymes; and Low Platelet count. A disorder if not treated quickly leads to death. The doctor emphasized the need for a quick response to the symptoms told to her.
This is only a brief recital of the tragedy which befell Lauren Bloomstein and her husband Larry. With additional delays in finding a surgeon, Lauren began to experience bleeding in her brain which would lead to paralysis. She knew she was dying before her husband’s eyes. A neurosurgeon was called in to relieve the pressure and stop the bleeding. Since her platelets were low he could not operate, the hospital did not have an adequate supply, and by the time additional supply arrived it was too late. Lauren was brain dead. She pass on after her daughter was placed next to her one last time.
What was Missed
The warning signs of life-endangering problems were there. Missed were the reoccurring pain in the kidney area or ignored indicating abnormal high blood pressure for Lauren. Excuses were given. Reflux for the pain and administering pain killers to dull the pain. Other symptoms (blood pressure) not explored while she deteriorated in front of her husband who suspected preeclampsia. The missing part of this was the protocol to diagnose early on and prevent Lauren from slipping into late stages of preeclampsia.
This was not an isolated incidence as the deaths of women giving birth keep increasing as evidenced in the attached chart.
This is but one story as told by NPR and Propublica. There are many more stories of tragedy which go untold. In this case, the doctor husband alerted the New Jersey Department of Health’s licensing and inspection division, which oversees hospital safety and filed a complaint.
After examining Lauren’s records, interviewing her caregivers and scrutinizing the hospitals policies and practices the DOH issued a report. In December 2012 it issued a report backing up everything Larry had seen first-hand.
Investigators found; “There was no notes in the medical record of the Registered Nurse notifying [the ob/gyn] of the elevated blood pressures of patient prior to delivery. There was no evidence in the medical record of further evaluation and surveillance of patient from [the ob/gyn] prior to delivery. And, there was no evidence in the medical record that the elevated blood pressures were addressed by [the ob/gyn] until after the Code Stroke was called.”
The report faulted the hospital. “The facility is not in compliance.” Too little, too late. Denying women, the right to abortion can and will cause serious issues with future health and even death. And the politicians in Mississippi will go home and have dinner.