Part 2 discusses why we must have the government issue payments to hospitals, clinics, etc. and also set the budgets for hospitals and this is how they are paid rather than billing multiple insurers and also patients. There is also only one payer. The later part is what I have been pounding on repeatedly. Forget prices and work with cost data. It is then we have a much clearer picture of the costs of healthcare and we can begin to control prices. Rep Jayapal and Sen Sanders Have Introduced Medicare For All Bills: One Is a Lot Better Than the Other, Healthcare for All Minnesota, Kip Sullivan, May 8, 2019 What is an ACO and why is it a defect? Congress included in the Affordable Care Act of 2010 (aka Obamacare) a section (Section 3022) requiring CMS to
Topics:
run75441 considers the following as important: Healthcare, Hot Topics, Journalism
This could be interesting, too:
NewDealdemocrat writes JOLTS revisions from Yesterday’s Report
Joel Eissenberg writes No Invading Allies Act
Bill Haskell writes Families Struggle Paying for Child Care While Working
NewDealdemocrat writes January JOLTS report: monthly increases, but significant downward revisions to 2024
Part 2 discusses why we must have the government issue payments to hospitals, clinics, etc. and also set the budgets for hospitals and this is how they are paid rather than billing multiple insurers and also patients. There is also only one payer. The later part is what I have been pounding on repeatedly. Forget prices and work with cost data. It is then we have a much clearer picture of the costs of healthcare and we can begin to control prices.
Rep Jayapal and Sen Sanders Have Introduced Medicare For All Bills: One Is a Lot Better Than the Other, Healthcare for All Minnesota, Kip Sullivan, May 8, 2019
What is an ACO and why is it a defect?
Congress included in the Affordable Care Act of 2010 (aka Obamacare) a section (Section 3022) requiring CMS to establish an ACO program within the traditional FFS Medicare program. It is not clear why Congress chose to use ACOs. Congress was warned in 2008 by the Congressional Budget Office (CBO) that ACOs would not save money for Medicare. The simplest way to describe ACOs is to say they are HMOs in training. Like HMOs, they are corporations that own or contract with chains of hospitals and clinics; they have the equivalent of enrollees; they attempt to keep their “enrollees” from seeking care outside their networks; they bear insurance risk (that is, they are paid on a per-enrollee basis and in exchange are obligated to provide medically necessary services to their enrollees); and because they are risk-bearing organizations, they generate overhead costs similar to those created by traditional insurance companies.
More on ACOs and the absence of Single Payer budgets past the leap
In fact, precisely because ACOs resemble insurance companies, nearly half of them already have contracts with insurance companies to help them carry out insurance-related tasks. The largest insurance companies – Aetna, Humana, and United Healthcare, for example – are already deeply embedded in the ACO industry.
The only significant differences between ACOs and HMOs are (1) ACO “enrollees” are assigned to ACOs (usually without their knowledge) whereas HMO enrollees choose to enroll, and (2) HMOs bear all insurance risk while ACOs split the risk of loss or savings with another insurer (in Medicare’s case, risk is shared with the Medicare program). [5] Both of these differences are being eroded. Many ACOs are saying they should be allowed to enroll people so they can restrict enrollee use of out-of-ACO providers, and some influential ACO proponents are proposing that ACOs be paid premiums so they can absorb total losses and keep total profits.
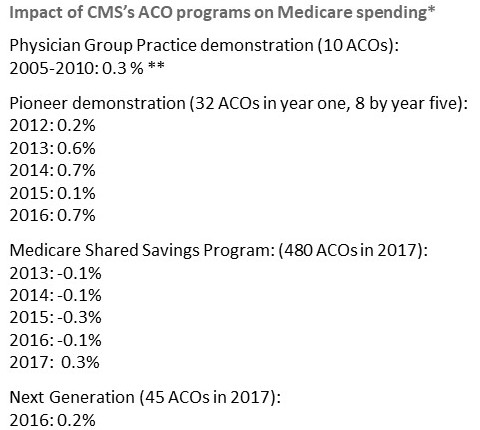
One other important similarity between ACOs and HMOs: ACOs have failed to cut Medicare’s costs, just as the CBO predicted. [6]
Defect 2: Absence of hospital budgets
I mentioned above that an American single-payer system could reduce total spending by 10 to 15 percent just by eliminating excess administrative costs. A large portion of that savings would come in the form of reduced administrative costs for hospitals (the rest comes from reduced administrative costs in the insurer and physician sectors). Hospitals enjoy lower overhead costs in single-payer systems for two reasons:
First, they are paid with annual budgets, not on a per-patient or per-procedure basis, which means they don’t have to keep track of every pill and x-ray for every patient.
Second, for the covered services, they deal with only one payer, not hundreds, each with their own hoops to jump through.
Unlike Representative Jayapal’s bill, Senator Sanders’ bill does not authorize hospital budgets. There is a reason for that: It is not possible to set premiums for 1,000 or 2,000 ACOs, which consist of hospital-clinic chains with an insurance company or department plopped on top of it, and at the same time set budgets for each of the nation’s 5,500 hospitals. One has to choose one or the other: Premium payments for ACOs, or budgets for hospitals. Sanders chose ACOs. Jayapal chose hospital budgets.
But by sacrificing hospital budgets in order to make room for ACOs, Sanders guaranteed his bill cannot reduce hospital administrative costs much or at all. Research indicates US hospitals spend 25 percent of their revenues on administration, thanks to the complexity of our multiple-payer system, while hospitals in single-payer systems that use hospital budgets devote half as much to administrative costs.
We must take into account as well the additional administrative costs for doctors in Sanders’ proposed multiple-ACO system. Like hospitals, they will have to determine, for each patient, which ACO a patient belongs to and send the bill to the right one.
Cost containment must accompany or precede universal coverage
If you happen to believe that some fine day America will find the political will to insure everyone at the high price at which health care is sold today, then you should ignore what I have said here. You should feel free to endorse any legislation that proposes to raise taxes high enough, or levy compulsory premium payments high enough, to achieve universal coverage. No need to worry about whether a bill that purports to achieve universal coverage can reduce costs. No need to ask yourself why US per capita health care costs are double those of the rest of the industrialized world. The answer is: Primarily because of our high prices, and the excessive administrative costs generated by our multiple-payer system that drive prices up, and not “overuse” of medical services.
But if you think, as I do, that cost containment must accompany or precede universal coverage, then you must support legislation that includes evidence-based, cost containment provisions, such as Representative Jayapal’s bill. I do not believe our nation will find the political will to pay for universal coverage at today’s prices. Moreover, even if the political will were there, I don’t believe it is ethical to pay more to solve any social problem than we have to. Our society has numerous other demands on our resources, ranging from hunger to crumbling infrastructure to climate change. Paying more than necessary to ensure all Americans means we will have fewer resources left with which to address other problems.
Representative Jayapal’s bill, HR 1384, meets the definition of a single-payer bill as originally outlined in PNHP’s 1989 article and as most experts define the term. It contains the four elements of a single-payer system:
- It relies on one payer (HHS, not multiple payers called ACOs) to pay hospitals and doctors directly,
- it authorizes budgets for hospitals,
- it establishes fee schedules for doctors,
- and it has price ceilings on prescription drugs.
Senator Sanders’ bill contains two of those four elements – fee schedules for doctors and limits on drug prices. That’s a good start. He should add the other two. He should get rid of Section 611(b), the section that authorizes ACOs, and thereby ensure HHS is the single payer. And he should add a section authorizing HHS to negotiate budgets with each of the nation’s hospitals.
(Kip Sullivan is a member of the Health Care for All Minnesota Advisory Board and of the Minnesota chapter of Physicians for a National Health Program.)
Footnotes for Part Two