Dan sent this article to me and I scan-read it as it is done in generalities. This not a criticism of the content as much as my pointing out it is done in brevity. The push is big for some form of Single Payer healthcare if one were to call it “insurance.” At some point and with the implementation of Single Payer healthcare, insurance could conceivably disappear. Medicare for All Rallies in 50 Cities Show Big Support for Universal Health Care, TruthOut, C. J. Polychroniou, July, 2021 “What keeps the country from adopting a universal health care system, which most Americans have supported for many years now? Peter Arno: The short answer as to why the U.S. has the highest health care expenditures in the world is simply that, unlike other
Topics:
run75441 considers the following as important: Healthcare, Hot Topics, Medicare4All, politics, Taxes/regulation, US EConomics
This could be interesting, too:
Robert Skidelsky writes Lord Skidelsky to ask His Majesty’s Government what is their policy with regard to the Ukraine war following the new policy of the government of the United States of America.
NewDealdemocrat writes JOLTS revisions from Yesterday’s Report
Joel Eissenberg writes No Invading Allies Act
Ken Melvin writes A Developed Taste
Dan sent this article to me and I scan-read it as it is done in generalities. This not a criticism of the content as much as my pointing out it is done in brevity. The push is big for some form of Single Payer healthcare if one were to call it “insurance.” At some point and with the implementation of Single Payer healthcare, insurance could conceivably disappear.
Medicare for All Rallies in 50 Cities Show Big Support for Universal Health Care, TruthOut, C. J. Polychroniou, July, 2021
“What keeps the country from adopting a universal health care system, which most Americans have supported for many years now?
Peter Arno: The short answer as to why the U.S. has the highest health care expenditures in the world is simply that, unlike other developed countries, we have very few price constraints on our health care products and services, ranging from drugs, medical devices, physician and hospital services to private insurance products. On a broader level, the corporatization and profits generated from medical care may be the most distinguishing characteristics of the modern American health care system. The theology of the market, along with the strongly held mistaken belief that the problems of U.S. health care can be solved if only the market could be perfected, has effectively obstructed the development of a rational, efficient and humane national health care policy.
Despite the U.S.’s outsized spending on health care, its relatively poor health outcomes are beyond dispute. For example, in 2019, the U.S. ranked 36th in the world in terms of life expectancy at birth — behind Slovenia and Costa Rica, not to mention Canada, Japan and all the wealthy countries in Europe. This is not solely, as one might at first think, a function of racial and ethnic health disparities, as dramatic as they are in the U.S. A recent study found that even white people living in the nation’s highest-income counties often have worse health outcomes on infant mortality, maternal mortality, and deaths after heart attack, colon cancer and childhood leukemia than the average citizens of Norway, Denmark, and other wealthier countries.
The relatively poor health outcomes in the U.S. require a more nuanced explanation based on income, wealth and power inequalities. These factors drive inadequate and inequitable access to health care. But they also undermine many of the social determinants of health, particularly for poor and vulnerable populations, which fall largely outside the health care sector. These include, for example, higher income, access to healthy food, clean water and air, adequate housing, safe neighborhoods, etc.”
I have written on healthcare, hospitals and pharmaceuticals a numbers of time discussing the costs (or pricing) paid by patients whether it comes in the form insurance payment, deductibles, copays, out-of-pockets, etc. Healthcare is expensive.
While Dr. Arno is calling for pricing constraints, I would take it much further and look at healthcare costs, examine them, and begin to measure them against the costs of manufacture and bringing them to market.
There is a move afoot to assess new uses of drugs and assigning a value to it as a measure of what it brings to market in healthcare improvements. The ICER evaluates the claims made by companies for new uses of drugs the same as it does with the introduction of new drugs. In 2019, I had written about such an exercise for nine drugs of which two drugs were found to have justifiable price increases for those drug based upon limited information provided,
I find the increase in pricing for old drugs used for new treatments to be provoking as little or no resources have been applied beyond R&D and the manufacturing ability is little more than sunk costs already paid. Profits are still accumulated.
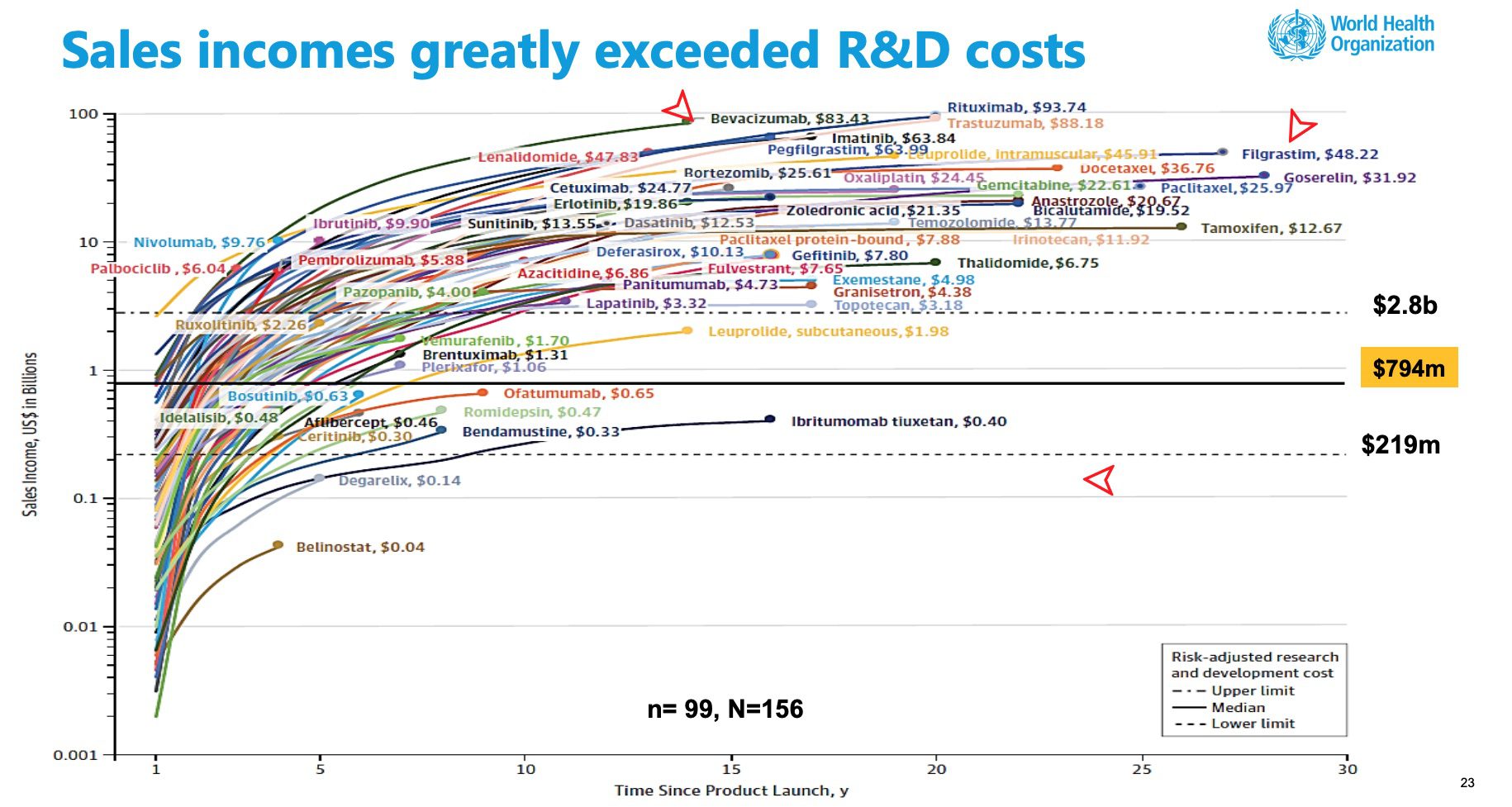
The WHO report establishes, Pharma companies do recoup their costs in a short period of time.
As the World Health Organization pointed out in “Pricing of Cancer Medicines and its Impacts“
The median time to generate revenue to fully cover risk-adjusted R&D cost of US $794 million was 3 years (range: 2 years; 5 years, n=73). For the maximum estimated risk-adjusted cost of R&D (US$2 827million), the time to cost recovery was 5 years (range: 2 years; 10 years, n=56).
Pricing of Cancer Medicines and its Impacts, WHO Technical Report, Page 26
Pricing of Cancer Medicines and its Impacts, WHO Technical Report, Page 26
To finally get to my point, we should be examining the costs of process, production, and materials. We should be doing this before setting a suitable price. Setting prices without knowing costs is little better than a dart throwing. Then too, why are we still paying list price after recouping all costs?
More on this as I spend time explaining today’s Medicare and Single Payer.