Summary:
Medicare Advantage Overbilling Taxpayers by 0 Billion a Year, This is Enough to Wipe Out Medicare Premiums, Informed Comment, Juan Cole and Jake Johnson.
AB‘s Joel sent me an Informed Comment article. I read the article and knew there was more to the issue than just overcharging the government by upcoding Medicare Advantage plan members. Merrill Goozner writes GoozNews and got the jump on this topic before me in March of this year. Catching up on the issue of overpayments to Medicare Advantage Plans. A lot of information which should help in understanding the problems with Medicare Advantage.
~~~~~~~~
Physicians for a National Health Program (PNHP) starts off by defining two issues with Medicare Advantage. To project the monetary size of
Medicare Advantage Overbilling Taxpayers by $140 Billion a Year, This is Enough to Wipe Out Medicare Premiums, Informed Comment, Juan Cole and Jake Johnson.
AB‘s Joel sent me an Informed Comment article. I read the article and knew there was more to the issue than just overcharging the government by upcoding Medicare Advantage plan members. Merrill Goozner writes GoozNews and got the jump on this topic before me in March of this year. Catching up on the issue of overpayments to Medicare Advantage Plans. A lot of information which should help in understanding the problems with Medicare Advantage.
~~~~~~~~
Physicians for a National Health Program (PNHP) starts off by defining two issues with Medicare Advantage. To project the monetary size of the issue, PNHP states the overcharges funded by Medicare could conceivably fund certain parts of traditional Medicare (see chart below).
“1. By our estimate, and based on 2022 spending, Medicare Advantage overcharges taxpayers by a minimum of 22% or $88 billion per year, and potentially by up to 35% or $140 billion.
2. By comparison, Part B premiums in 2022 totaled approximately $131 billion, and overall federal spending on Part D drug benefits cost approximately $126 billion.
Either of these (1 or 2 above) or other crucial aspects of Medicare and Medicaid could be funded entirely by eliminating overcharges in the Medicare Advantage program.”
MA Overpayment Report, pnhp.org, Physicians for a National Health Program
Managed care cheerleaders maintain programs like MA reduce expenditures, improve the quality of care and enable consumer choice. The reality is the opposite as data shows, privatized Medicare has not once yielded savings for the program. Each year MedPAC (Medicare Payment Advisory Commission) an independent agency issues a report to Congress on the Medicare Program showing (2022 and 2023):
1. The conservative estimates by MedPAC show payments to MA plans over the past two decades have always been higher then would have been for patients in Traditional Medicare.
2. Despite this additional spending, MedPAC could not say conclusively whether care outcomes fared better under MA.
3. Patients in Traditional Medicare have access to nearly all doctors and hospitals across the country
4. Patients in Medicare Advantage plans must contend with heavily limited networks.
5. Healthcare is further limited by arcane prior authorization procedures, calling into question which choices consumers are able to make.
The MedPAC report for 2022 reveals the variances in coding incurred by Medicare Advantage. Chapter 12, Page 439, Report to the Congress: Medicare Payment Policy | March 2022. “Coding differences increased payments to MA plans by $12 billion in 2020.” Yearly variances as reported by MedPAC (bar chart);
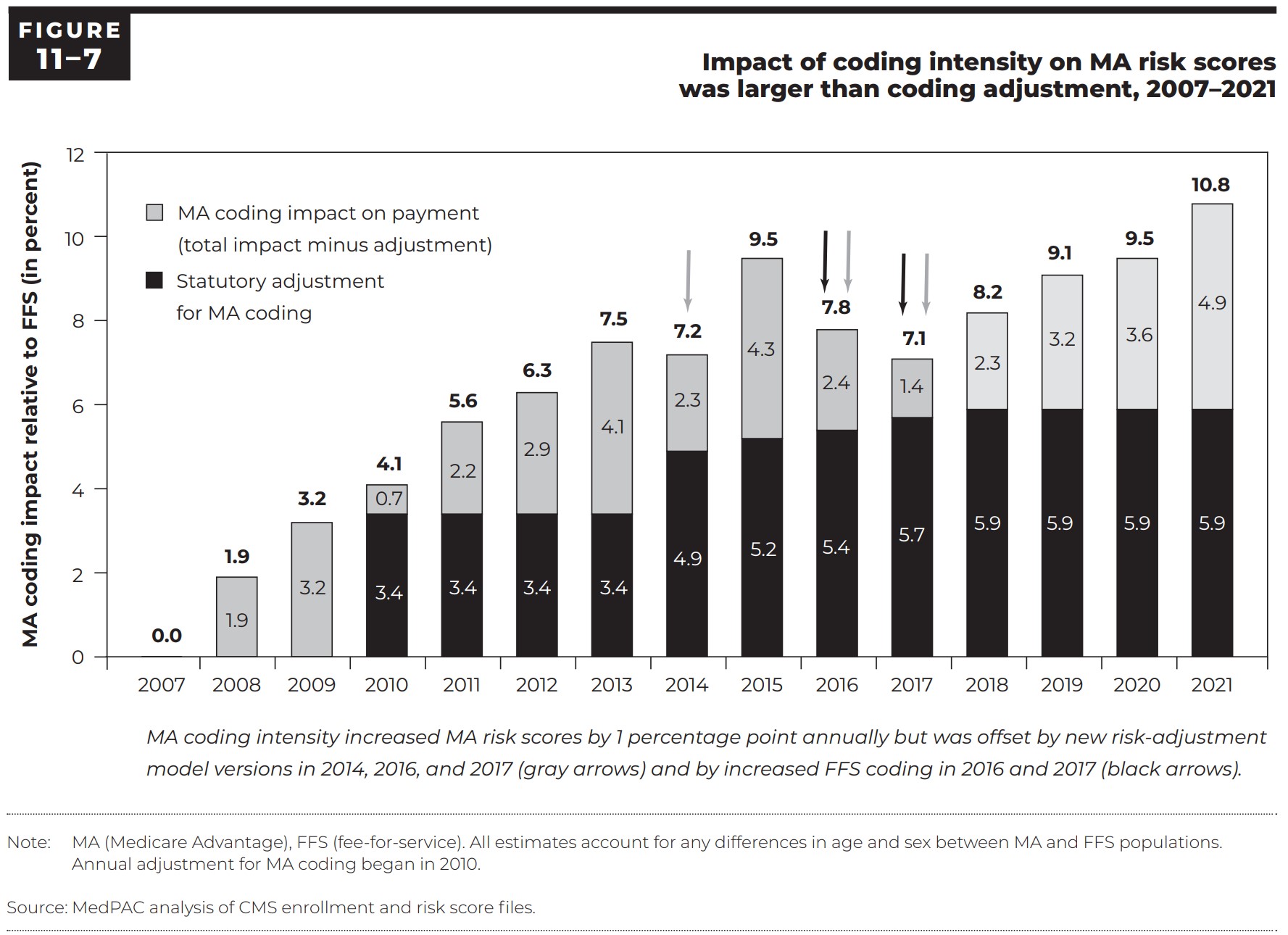
“Figure 12-6, Payment years 2007 through 2020 (14 years).” The impact of differences in coding intensity (increasing codes) on MA risk scores in relation to FFS plus the size of the coding intensity adjustment (the amount by which CMS reduced MA risk scores to account for coding intensity) is what we are looking at today. During the 2007 -2020 period, coding intensity consistently increased MA risk scores by approximately one percentage point or more annually.
However, the underlying trend was offset in 2014, 2016, and 2017 by the introduction of new versions of the risk-adjustment model and more intensive FFS coding. The coding intensity adjustment has never fully accounted for the impact of coding intensity. This difference results in continuing excess payments to MA plans relative to FFS spending for similar enrollees.
For 2020, MA risk scores were 9.5 percent above FFS risk scores. The difference was partially offset by the coding intensity adjustment reducing MA risk scores by 5.9 percent. The net effect was a 3.6 percent increase in MA risk scores, leading to nearly $12 billion in excess payments to MA plans. The magnitude of these findings is consistent with most other research showing that the impact of coding differences on MA risk scores is larger than CMS’s adjustment for coding.”
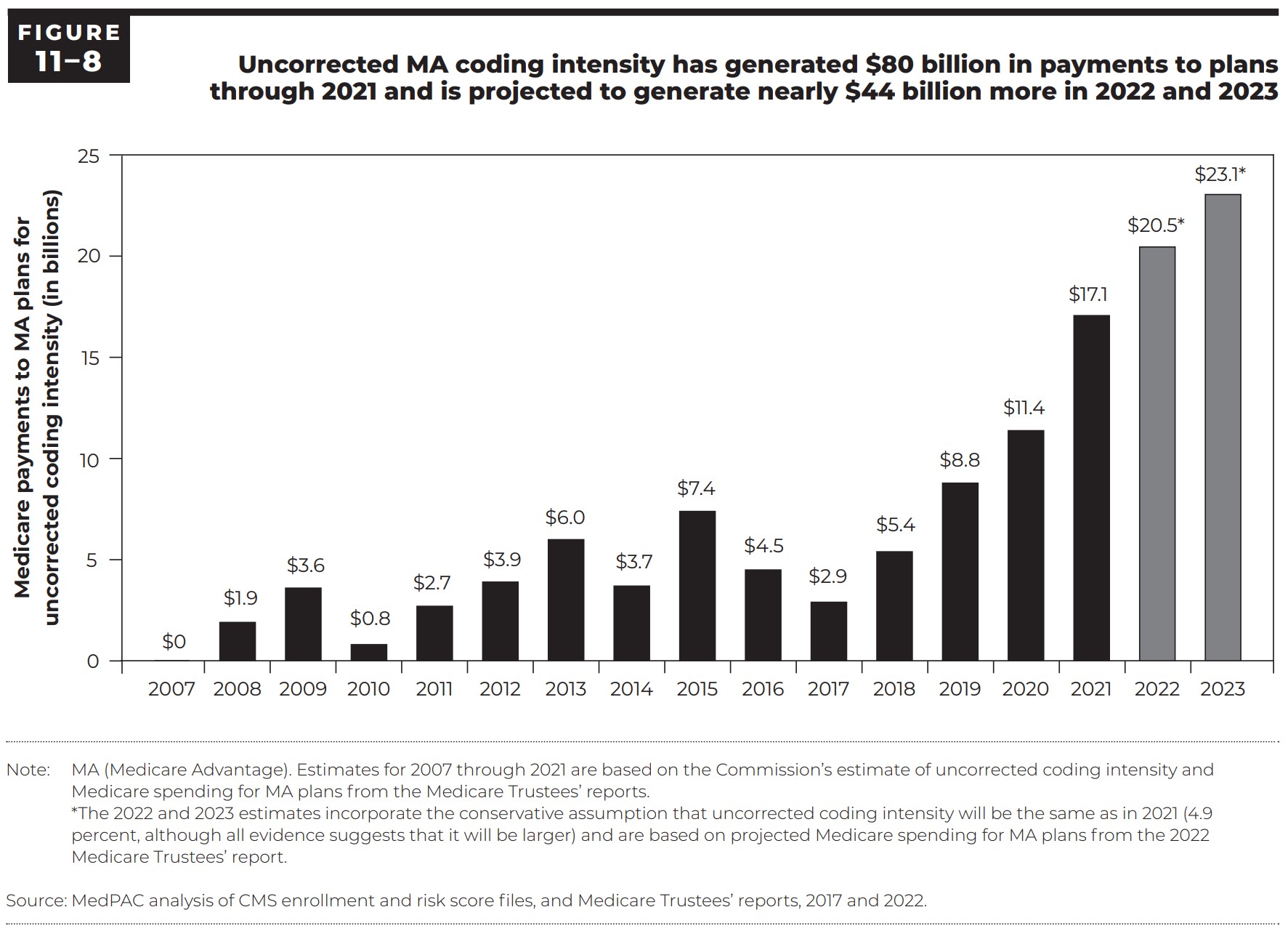
The following year there was another increase in expenditures due to over coding. In 2021, the coding differences increased payments to MA plans by $17 billion.
Inflated MA payments due to coding differences have been under scrutiny for more than a decade. Starting in 2010, a series of congressional mandates required CMS to reduce MA risk scores to address the impact of MA and FFS coding differences on payments to MA plans. Because of these mandates, CMS reduced MA risk scores by 3.41 percent in each year from 2010 through 2013. As you can see in the graph above MA coding increasing coding occurs from 2018 to 2021.
Starting in 2014, legislation specified a minimum reduction of about 4.9 percent, which rose gradually to about 5.9 percent in 2018, where it will remain until the Secretary of Health and Human Services implements risk adjustment using MA diagnostic, cost, and use data. Although larger reductions are allowed under the legislation, CMS reduced MA risk scores by only the minimum amount required by law for 2014 through 2023. In 2023, CMS will again reduce MA risk scores by 5.9% of the 10.8% coded by MA plans. This is a 2.6% increase since 2018 (fig. 11-7above). But what of the $88 to $140 billion in claimed Medicare Advantage billings to Medicare?
In the latest MedPAC Report, figure 11-8 on page 354 gives part of the answer as to where the $88 – $140 billion increase Jake Johnson at Informed Comment is talking about in “Medicare Advantage Overbilling Taxpayers by $140 Billion a Year — Enough to Wipe Out Medicare Premiums,” Juan Cole (juancole.com).
In the latest MedPAC March 2023, the estimated “upcoding” amount is $23.1 billion for 2023. This chart was not in the prior MedPac Report for prior years I had used to write an earlier report on Medicare Advantage. This is only a part of the $88 – $140 billion increase for Medicare Advantage everyone is talking about. Where is the rest of it? Glad you asked.
Informed Comment (Jake) gives us another link. This time it links to a report “MA Overpayment Report” (pnhp.org). I did read the report and found another chart which fleshes out the other items making up the rest of the $88 – $140 billion increase for Medicare Advantage.
MA Overpayment Report, pnhp.org, Physicians for a National Health Program
Terminology of Overpayment Sources:
Favorable Selection: We (MA) want only the healthy ones which can be up-coded. If ill? Eventually, you will be priced out. More than likely, Supplemental insurance may not be available to you upon your return to traditional FFS Medicare.
County Benchmarks and Quality Bonus: Benchmark is the maximum amount the federal government will pay for a Medicare Advantage enrollee and is a percentage of estimated spending in traditional Medicare in the same county, ranging from 95 percent in high-cost counties to 115 percent is low-cost counties. Plans receiving at least four (out of five) stars have their benchmark increased. Quality Bonus: For most plans in bonus status, the benchmark is increased by five percentage points. Plans in “double bonus” counties (defined as urban counties with low traditional Medicare spending and historically high Medicare Advantage enrollment) have their benchmark increased by 10 percentage points. In addition, the benchmarks for plans without ratings due to low enrollment or being too new are increased by 3.5 percentage points.
The term Induced Utilization warrants clarification. The term “Induced utilization” from an article by Richard Gilfillan and Donald Berwick refers to the idea people with MA supplemental coverage are likely to use more health care because their insurance pays for more of their cost thereby removing some of the financial barriers to accessing health services. In this case, given the difference described in Gilfillan and Berwick’s article, the average rebate amount from induced utilization would be approximately $108 per beneficiary per month.
The issue here is the over coding by Medicare Advantage plans for the upcoming year or it could be denial of care after coding. In both cases Medicare Advantage is paid. Medicare Advantage can not compete head to head with Traditional Medicare. The latter is not allowed to offer the same benefits as Medicare Advantage. The funding of Medicare Advantage is depleting Traditional Medicare reserve funds. If Medicare Advantage was forced to compete head-to-head with Traditional Medicare, it would lose as it is more expensive.
There is something better than FFS about which Berwick once said:
“20 to 30 percent of health spending is ‘waste’ that yields no benefit to patients, and that some of the needless spending is a result of onerous, archaic regulations enforced by Medicare and Medicaid.
He listed five reasons for what he described as the ‘extremely high level of waste.’ They are overtreatment of patients, the failure to coordinate care, the administrative complexity of the health care system, burdensome rules and fraud.
Much is done that does not help patients at all and many physicians know it.”
Joe Biden: “How Are We to Pay for Single Payer Healthcare Alias Medicare for All?” Angry Bear.
Single Payer brings with it greater efficiencies and lowers costs due to the former.
Sources . . .
Medicare Advantage Overbills Taxpayers by $140 Billion a Year — Enough to Wipe Out Medicare Premiums, Informed Comment, Juan Cole and Jake Johnson.
MA Overpayment Report, pnhp.org, Physicians for a National Health Program.
How Medicare Advantage Plans Dodged Auditors and Overcharged Taxpayers by Millions, KFF Health News, Fred Schulte and Holly K. Hacker