The issues being addressed in the second part of the Center for Healthcare Quality and Payment Reform or CHQPR ORG, report reviews what is causing small rural hospitals to close. Provided is also glimpse at a solution to fix and maintain small rural hospitals which can not maintain the necessary facility and service to local patients on their own. This is a patient-focused approach using a funding scheme designed to support the services patients need and facility required to provide them, It does not increase profits for either hospitals or health insurance plans. The report suggests a core solution being a fee plan in support of the costs services or utility are 10% utilized or not. The issue is the fixed costs of staff to man the ED,
Topics:
run75441 considers the following as important: Healthcare, Rural Hospitals
This could be interesting, too:
Bill Haskell writes Families Struggle Paying for Child Care While Working
Joel Eissenberg writes RFK Jr. blames the victims
Joel Eissenberg writes The branding of Medicaid
Bill Haskell writes Why Healthcare Costs So Much . . .
The issues being addressed in the second part of the Center for Healthcare Quality and Payment Reform or CHQPR ORG, report reviews what is causing small rural hospitals to close. Provided is also glimpse at a solution to fix and maintain small rural hospitals which can not maintain the necessary facility and service to local patients on their own.
This is a patient-focused approach using a funding scheme designed to support the services patients need and facility required to provide them, It does not increase profits for either hospitals or health insurance plans. The report suggests a core solution being a fee plan in support of the costs services or utility are 10% utilized or not.
The issue is the fixed costs of staff to man the ED, Radiology, Labs and similar departments which may not be utilized as frequently as other parts of a small hospital. Present utilization does not cover costs, So, how do you fix it? Change your pricing for these parts of the hospital to recoup to a breakeven status. The other problematic part of this is lower payments from insurance companies, Medicare Advantage, Medicaid, etc. Other service profit can not cover the costs of them.
It is a good read. Tried to shorten it and was unable to impact it to make a difference. This is the Part 11 of the earlier commentary on Rural hospitals. “Small Town and Rural Hospitals Are at Risk of Closing due to Funding,” Angry Bear.
Better Way to Pay Rural Hospitals, Center for Health Quality and Payment Reform
There are over 1,000 small rural hospitals in the U.S., representing more than one-fourth of the short-term general hospitals in the country. Small rural hospitals deliver traditional hospital services such as emergency care, inpatient care, and laboratory testing. Most of them also deliver primary care and inpatient rehabilitation services. The communities they serve can be at least a half-hour drive from the nearest alternative hospital. In many cases, there are no other sources of health care in their community.
More than 600 rural hospitals or nearly 30% of all rural hospitals in the country are at risk of closing in the near future. Over 200 of these hospitals are at immediate risk of closure. Harm could come to millions of people if rural hospitals close. The rest of the country would also be affected through the impacts on workers in agriculture and other industries.
Small rural hospitals are forced to close due to being paid less than what it costs to deliver care in rural areas. While most urban hospitals and larger rural hospitals make profits on patient services, many small rural hospitals lose money delivering services to patients. The biggest cause of these losses is inadequate payments from private insurance plans. Large hospitals can offset losses on Medicaid and uninsured patients with the profits they make on patients with private insurance, small rural hospitals cannot.

The Cost of Delivering Essential Hospital Services
Understanding the problems with current payments requires understanding the differences between fixed costs, variable costs, and average costs in the delivery of healthcare services:
- Fixed Costs. Hospitals have to have to have a minimum level of
personnel and equipment in order to ensure it can deliver time-sensitive services to patients when needed. The most obvious example of this is the hospital Emergency Dept, (ED). Small hospitals need to have at least one physician and nurse available on a 24/7 basis in order to promptly diagnose and treat patients when they come to the ED. Other hospital departments, such as the laboratory and radiology, also have to be available around the clock to preform basic tests and imaging studies for patients who come to the ED. This minimum number of personnel need to be “standing by” to deliver services every hour, even if there are no patients at all. This personnel standby capacity becomes a fixed cost for the hospital. The need does not decrease if fewer patients come to the hospital over the course of the year. - Variable Costs. The hospital will incur additional costs when a patient does come to the hospital for a service (e.g., the cost of supplies and drugs used for diagnosis and treatment). It will also incur additional personnel costs if the number or types of patients needing services is more than what can be handled with the minimum level of staffing in the ED, laboratory, or inpatient unit. These are variable costs for the hospital. They increase or decrease based on the number of patients and the types of services delivered.
- Total Costs. The total cost of providing a particular type of service (e.g., Emergency Department visits or inpatient care) is the sum of the fixed costs and the variable costs. The total payments the hospital receives for the services must be greater than the total cost of delivering them. Since the variable costs depend on the number of services delivered, the total cost will be higher if the service is delivered more frequently, and so more revenue will also be needed. If no patients use the ED, the cost of the staff and the unit still exists.
- Average Cost. The average cost of a service is equal to the total cost incurred in delivering the service over a period of time (e.g., a year) divided by the number of services delivered during that period of time. Since the fixed costs do not depend on the number of services delivered, the average cost of a service will increase if fewer patients need the service, and vice versa. The average cost of an essential service is higher at a smaller rural hospital than at a larger hospital because the fixed cost is the same, even though the volume of services is lower.
The Problems Caused by Current Fee-for-Service Payments
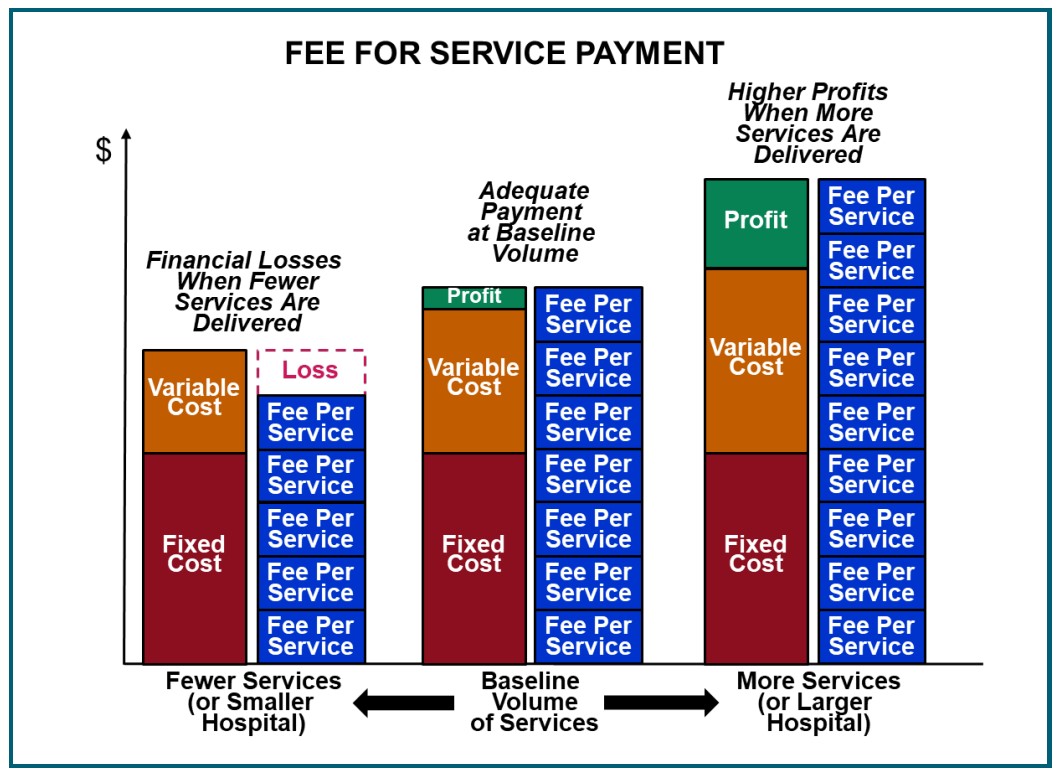
Under a standard fee-for-service payment systems, a hospital is paid a fee each time it delivers a service to a patient (e.g, an Emergency Department visit, laboratory test, or imaging study). In theory, the fee should equal the average cost of delivering each service, so the hospital will receive just enough revenue to cover the total cost of delivering services during the year.
However, because of the high fixed cost of delivering essential services, the average cost depends on the number of patients who need the service. As a result, the average cost will almost always be higher or lower than a preset fee. This means:
- Higher profits for the hospital will result if more services are rendered. The average cost of the service will decrease, and the revenue from the fees will be higher than the total cost.
- Higher losses for the hospital if patients need fewer services. Conversely, if the hospital does not need to deliver as many services, the average cost of delivering a service will increase because only the variable costs will decrease, not the fixed costs. If the fee for each service stays the same, total revenues will fall short of the total cost, causing a loss.
If small rural hospitals are paid the same fees for services as larger hospitals, the small rural hospitals will lose money. Many insurance companies actually pay small rural hospitals less than they pay larger hospitals for the same services Even though the average cost of delivering the services at the small hospital will be higher.
If a small hospital provides primary care and other services designed to help patients stay healthy, the number
of ED visits and treatment services at the hospital is likely to decrease. This too can increase financial losses for the hospital.
Small rural hospitals designated as Critical Access Hospitals are paid by Medicare based on the actual cost of
their services instead of the standard fees paid to larger hospitals, Those payments will increase if fewer patients need services during the year. The big however here being commercial health insurance plans, Medicare Advantage plans, and most Medicaid programs pay for services using standard fees. The majority of revenues at Critical Access Hospital still come from fee-for service payments. Moreover, under current federal sequestration rules, the “cost-based” payments from Medicare are only 99% of the average cost of services, so a Critical Access Hospital is forced to lose money even on services to Original Medicare patients.
Since current payment systems do a poor job of supporting the delivery of high-quality healthcare in rural areas, a better method for paying small rural hospitals is needed. However, just because a payment system is different does not make it better. The weaknesses in current systems need to be corrected while also preserving their strengths.
Patient-Centered Payments for Rural Hospitals
Goals for a Successful Payment System
A good payment system should achieve three key goals:
- Ensure availability of essential services in the community. A rural community needs to have assurance the hospital’s emergency department and basic diagnostic and treatment services will be available to deliver high-quality services at all times.
- There is a minimum cost involved in providing this capacity in a small community. The hospital needs to have sufficient revenue to cover the cost, regardless of how many people actually have emergencies or illnesses requiring diagnosis and treatment. Payments based solely on the number of services delivered may not generate sufficient revenues to cover this “fixed cost” and an arbitrary global budget may also fail to do so also.
- Enable timely delivery of the services patients need. When community residents have health problems, payments should enable the hospital to provide appropriate diagnostic and treatment services as quickly and efficiently as possible. The hospital should not be prevented (lack of capability) from delivering services to all patients who need them by an arbitrary cap on its revenues, nor should it be paid the same amount even if it delivers fewer services than patients need, which is what would happen under a global budget. Moreover, insurance plans should not discourage or prevent patients from obtaining high-quality care by requiring high cost-sharing amounts or refusing to pay for services at the community hospital.
- Support delivery of appropriate, high quality, affordable care. Hospitals should be paid adequately to deliver services safely, efficiently, and in ways evidence indicates will achieve good outcomes. The payment system should not reward hospitals for delivering unnecessary services or for charging prices higher than necessary. Nor should it financially penalize hospitals for preventing complications and improving patient outcomes, as happens under the fee-for-service system. The payment system should also not reward a hospital for reducing access to services for patients or pay the hospital even when it delivers low quality care, as a global budget would.
Components of a Successful Payment System
Achieving all three of these goals requires a payment system with four components:
- Standby Capacity Payments to Support the Fixed Costs of Essential Services. The hospital should receive a Standby Capacity Payment for each person living in the community served by the hospital, regardless of how many services those people actually receive. These payments would be designed to pay for the minimum fixed costs required to adequately staff an emergency department, inpatient unit, and other essential service lines.
- Service-Based Fees for Diagnostic and Treatment Services Based on Variable Costs. The hospital should also receive a Service-Based Fee when a patient receives a specific service. This payment would only need to cover the variable costs of the service, since the minimum fixed costs would be paid for by the Standby Capacity Payments. As a result, the Service-Based Fees would be smaller than current fee for-service payments.
- Accountability for Quality and Efficiency. In return for receiving adequate payments, hospitals should be expected to deliver evidence-based services safely and efficiently.
- Value-Based Cost-Sharing for Patients. The amount a patient has to pay out of pocket to receive necessary services should be affordable for the patient, so patients are not prevented from obtaining the care needed to improve their health.

This is a patient-centered approach to payment because it is designed to support the services patients need and not increase profits for either hospitals or health insurance plans.
More details on each of these components are provided below.
Standby Capacity Payments to Support the Fixed Costs of Essential Services
The fee-for-service payment system includes fees for thousands of individual healthcare services. However, there is no fee at all for what residents of a rural community would likely view as the most important service of all – the availability of physicians, nurses, and equipment to diagnose and treat a serious health problem if the resident experiences an injury or illness.
Instead of being paid only for the patients who actually receive emergency, inpatient, or other services, the hospital also needs to be paid for each potential patient or each community resident who does not happen to need the ED or inpatient care during a particular month. They benefit from having those services available in case they do have such a need.
Communities do not force their fire department to support itself by charging high prices for extinguishing fires. Similarly, small rural hospitals should not be expected to pay for their emergency department by charging high prices for patients who need emergency care.
Standby capacity is an important healthcare service, because failure to provide it can result in worse outcomes and higher healthcare spending for residents of the community. Consequently, hospitals should receive Standby Capacity Payments from health insurance plans to pay for that capacity:
- All health insurance plans (Medicare, Medicare Advantage, Medicaid, and commercial insurance) should pay a Standby Capacity Payment for each of their members who live in the community served by the hospital. For each resident of the hospital’s service area who has health insurance, their insurance plan would pay the Standby Capacity Payment to the hospital each month. This per-member payment would be paid by the insurance plan in addition to Service-Based Fees for any individual services the insurance plan member receives if they go to the hospital for care.
- The hospital’s total revenue from Standby Capacity Payments should cover the fixed cost of adequate standby capacity. In the aggregate, Standby Capacity Payments from all payers should be sufficient to support the fixed costs of adequate staffing and equipment for the hospital’s Emergency Department services, laboratory and radiology services, basic inpatient care, and other essential services. The costs the hospital would have to incur even if only a small fraction of community residents actually need to use the services in any particular month.
A separate Standby Capacity Payment should be paid to a hospital if it delivers specific types of services (e.g., labor and delivery services or inpatient psychiatric services) to a broader service area. This enables the insurance plans for residents of other communities to pay to support the standby capacity needed for those specific services.
Conversely, a hospital should not expect to receive Standby Capacity Payments from health insurance plans for purely elective services, or if there are other providers already offering adequate access to a service in the same community.
Many rural communities currently use local taxes to cover the financial losses their hospitals incur delivering services to community residents. These local tax levies could be reduced if the hospital receives adequate Standby Capacity Payments from health insurance plans funded by the premiums local residents and businesses have already paid for health insurance.
Service-Based Fees for Diagnostic and Treatment Services Based on Variable Costs
By design, the Standby Capacity Payments will only be sufficient to support the minimum fixed cost of operating a service line. Consequently, the hospital will still need to charge Service-Based Fees in order to cover the additional, variable costs incurred when it delivers services to patients. These Service-Based Fees can be lower than the fees charged today because they will no longer need to cover the fixed costs of the service line; the fixed costs will be paid for by the Standby Capacity Payments.
Using two different types of payments to support essential services – a Standby Capacity Payment based on fixed costs, and Service-Based Fees based on variable costs – will do a much better job of matching the hospital’s revenues to its costs than either paying fees only when services are delivered or paying a single global budget regardless of how many services are delivered:
- If the amounts of Service-Based Fees are based on the variable cost of services, the hospital will not make significant profits by delivering more services nor will it incur significant losses when fewer services are delivered. Many hospitals charge high prices for all of their services and justify doing so based on the need to pay for standby capacity. Even though many of the services are not available on a 24/7 basis and even though the extra revenue generated through the higher charges may be far more than is needed to sustain the services that do need to be available on a round-the-clock basis. Paying directly to support standby capacity for essential services would enable more appropriate and affordable prices for individual hospital services.
- Using two different payments (the Standby Capacity Payment and the Service-Based Fee) is a more equitable way of charging patients (and their health insurance plans) for services than either traditional fees or global budgets, since patients who use more services will pay more but patients who need few services will still help to maintain the capacity required so they can receive services when they do need them.

If a health insurance plan is unwilling to pay Standby Capacity Payments for its members, it would be unfair for it to pay the same Service-Based Fees when its members receive services, since the plan would not be contributing to the fixed cost of the hospital’s services. These health plans (and their members) would need to pay higher Service-Based Fees when essential services are delivered to their members. Similarly, if tourists or non-residents who work in the community receive emergency services in the hospital, they would need to pay a higher fee, particularly if the hospital has to maintain a higher ED capacity to meet the needs of both residents and non-residents.

Accountability for Quality and Efficiency
In return for receiving adequate payments to support the cost of services, rural hospitals should take accountability for delivering high-quality care to patients. The “value-based payment” systems currently used by Medicare Advantage and other payers cannot and should not be used for small rural hospitals. Not only have these systems failed to significantly improve quality where they have been used, they are particularly problematic in rural communities because the quality measures do not produce statistically valid results for many types of rural residents and patients. Also rural hospitals cannot control the services physicians and hospitals in other cities will order or deliver for those patients who need specialized care the rural hospital cannot provide.
Instead, in order to participate in the Patient-Centered Payment system, the hospital should agree that it will only bill for a service if the service has been delivered in accordance with evidence-based Clinical Practice Guidelines (CPGs). If the hospital has to deviate from evidence-based guidelines for patient specific reasons (e.g., the patient was unwilling or unable to use the evidence-based treatment), the hospital would need to document those reasons in the patient’s clinical record in order to be paid for the services that were delivered.
In contrast to current pay-for-performance systems based on measures of average quality, this approach assures that each individual patient is receiving the most appropriate, high-quality care for their specific needs. It also eliminates the need for burdensome quality reporting systems that significantly increase administrative costs for both hospitals and payers. Moreover, since clinical practice guidelines define which services are inappropriate as well as which services are appropriate, they can reduce use of unnecessary services in a more patient-centered way than burdensome and problematic prior authorization processes operated by health plans.
Since the Standby Capacity Payments are designed to ensure that essential services are available when needed, in order to receive those payments, the hospital would need to document that the Emergency Department, laboratory, inpatient unit, and other standby services are staffed appropriately on a 24/7 basis.
Small Town and Rural Hospitals Are at Risk of Closing due to Funding, Angry Bear angry bear.