The following definitions I found in the article “What Kaiser’s Acquisition of Geisinger Means For Us All,” Forbes, Robert Pearl M.D. May 31, 2023 There are a couple of terms within the article which I would like to point out. Fee For Service and Fee For Value. For clarity, Traditional Medicare uses Fee For Service methodology and Medicare Advantage uses Fee For Value methodology. The following paragraphs were pulled from the Forbes article Question 3 “Will The Deal Work,” You are going to hear a lot about each manner of payment FFS and Capitulation (Fee For Value) and why each side giving healthcare thinks their methodology is better. Anything outside of Single Payer is commercial healthcare. Medicare sets fees and has its issues. ~~~~~~~~
Topics:
run75441 considers the following as important: Education, fee for service, Fee for Value, Healthcare, politics, US/Global Economics
This could be interesting, too:
Robert Skidelsky writes Lord Skidelsky to ask His Majesty’s Government what is their policy with regard to the Ukraine war following the new policy of the government of the United States of America.
Joel Eissenberg writes No Invading Allies Act
Ken Melvin writes A Developed Taste
Bill Haskell writes The North American Automobile Industry Waits for Trump and the Gov. to Act
The following definitions I found in the article “What Kaiser’s Acquisition of Geisinger Means For Us All,” Forbes, Robert Pearl M.D. May 31, 2023
There are a couple of terms within the article which I would like to point out. Fee For Service and Fee For Value. For clarity, Traditional Medicare uses Fee For Service methodology and Medicare Advantage uses Fee For Value methodology.
The following paragraphs were pulled from the Forbes article Question 3 “Will The Deal Work,” You are going to hear a lot about each manner of payment FFS and Capitulation (Fee For Value) and why each side giving healthcare thinks their methodology is better. Anything outside of Single Payer is commercial healthcare. Medicare sets fees and has its issues.
~~~~~~~~
Article: Most healthcare observers understand the inherent flaw in the “fee for service” (FFS) model is also its greatest appeal to providers: the more you do the more you earn. FFS is how nearly all financial transactions take place in America (i.e., provide a service, earn a fee). In medicine, however, this financial model results in frequent over-testing and over-treatment with minimal if any improvement in clinical outcomes, according to researchers.
AB: If you click on the link above, you end up here; Moving the Health Care System Away from Fee-for-Service, a short paragraph. There is not much there to discuss. So, I moved on to the links. If you click on the link “alternative payment, you end up at an article, “Wielding the Carrot and the Stick: How to Move the U.S. Health Care System Away from Fee-for-Service Payment,” Commonwealth Fund, Stuart Guterman, August 27, 2013. The first link in Gutterman’s paper “fail to provide incentives” does not link to anything. The second link “broad range” takes you to “100% of Americans agree: this page does not exist,’ but it might if we work together.” The third link, takes you a length paper “Bending the Curve: Person-Centered Health Care Reform – A Framework for Improving Care and Slowing Health Care Cost Growth,” Brookings, April 29, 2013 and no author that I can find. One out of the three links work and the articles linked to are a decade old. Much has transpired since 2013.
Article: The “value-based” alternative to FFS involves prepaying for care. A model often referred to as “capitation.” In short, capitation involves a single fee, paid upfront for all the medical care provided to a defined population of patients for one year based on their age and health status. The better an organization at preventing disease and avoiding complications from chronic illness, the greater its success in both clinical quality and affordability.
AB: The value-based plan in Medicare is called Medicare Advantage. Medicare Advantage evaluates each patient on a yearly basis (year 2022 valuation for year 2023) and submit the codes determined by the doctors within the Medicare Advantage plans to CMS MedPac. What has been happening over the years is the Medicare Advantage Commercial Insurance Plans has been over coding it patients. Medicare Advantage receives the payments and pays the doctors within their plans the same as commercial insurance is paid by Medicare.
Within Medicare, the cost of care is far less than the cost of commercial healthcare. The coding by Medicare Advantage Plans has lead to capitulation-over-coding. For year 2020, commercial insurance over coding results to Medicare.
Article: Within the small world of capitated healthcare payments, there’s an important element that often gets overlooked. It makes a big difference who receives that lump-sum payment.
In the case of Kaiser Permanente, capitated payments are made directly to the medical group and the physicians who are responsible for providing care. In almost every other health system, an insurance company collects capitated payments but then pays the medical providers on a fee-for-service basis. Even though the arrangement is referred to as capitated, the incentives are overwhelmingly tied to the volume of care (not the value of that care).
In a mixed-payment model, doctors and hospitals invariably prioritize the higher paying FFS patients over the capitated ones. When I think about these conflicting incentives, I’m reminded of a prominent medical group in California. It had a main entrance for its fee-for-service patients and a second, smaller one off to the side for capitated patients.
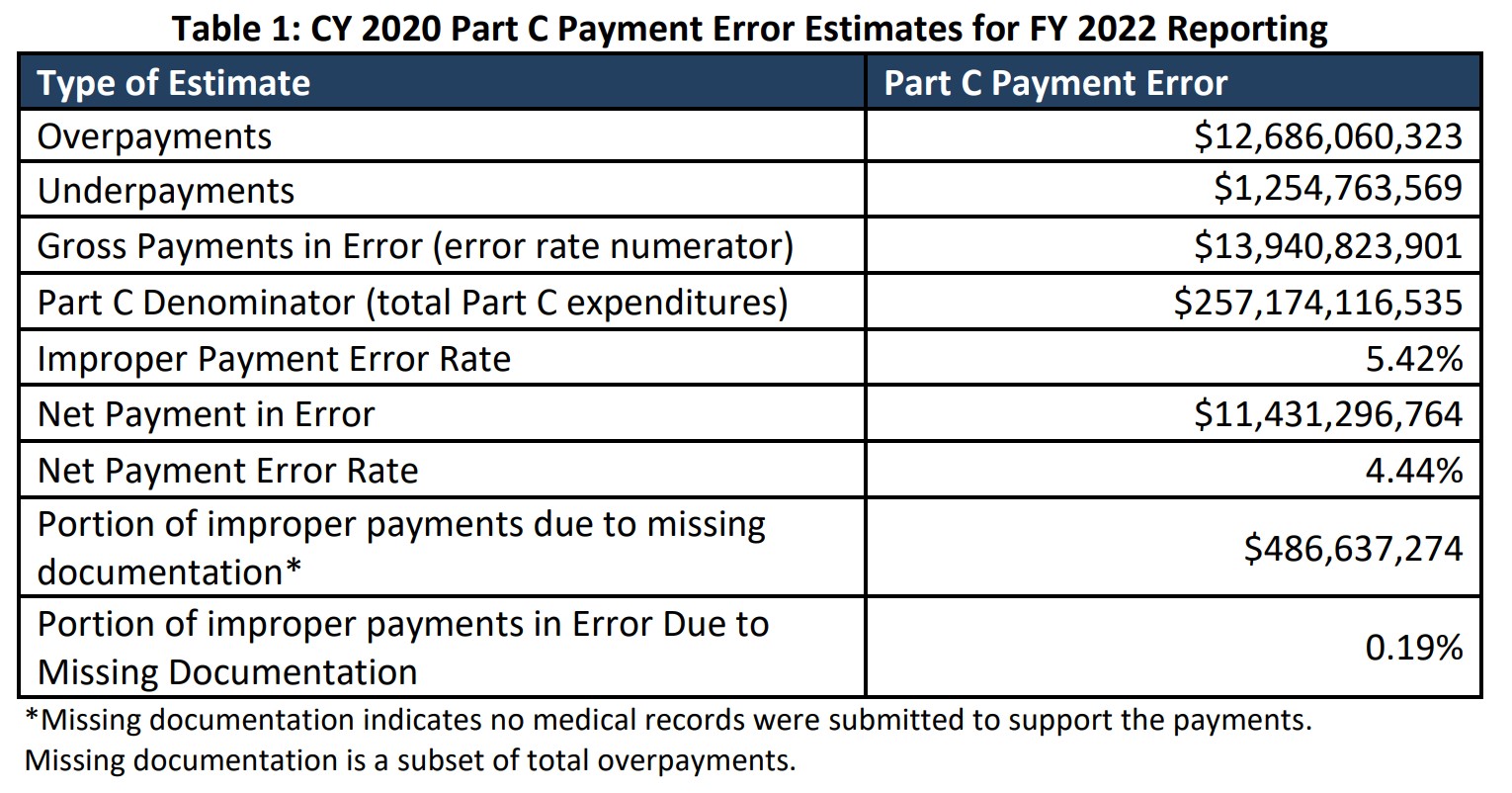
AB: In 2022, Kaiser suffered a $4.47 Billion Net Loss. Rising Costs are Blamed for Kaiser Permanente’s Net Loss. Now I have talked about Medicare FFS and Medicare Advantage Fee For Value costing. Most doctors would rather have patients with Medicare Fee For Service healthcare insurance because there is less chance of the rejection game being played. And it does happen quite frequently with Commercial Healthcare Insurance which Medicare Advantage is also. The only difference here is discovered over coding by Advantage plans resulting in overcharges of ~$12 billion in 2020. Furthermore, Medicare Advantage plan over coding is bleeding the Medicare trust fund rapidly.
A thought? Lets go to Single Payer healthcare and eliminate healthcare insurance. Single Payer will set rates and hospital budgets, etc.
Article: I doubt the time spent with the patient—or the overall care provided—was equal for both groups. When income is based on quantity of care, not quality, clinicians focus more on treating the complications of chronic disease and medical errors rather than preventing them in the first place. Geisinger has walked this tightrope in the past, but as economic pressures mount, I fear doctors will find the two sets of incentives conflicting and difficult to navigate.
AB: Lets code properly and not deny, deny coverage which is apparent in commercial healthcare insurance.
Bending the Curve: Person-Centered Health Care Reform – A Framework for Improving Care and Slowing Health Care Cost Growth,” Brookings, No author, April 29, 2013
Rising Costs Blamed For Kaiser Permanente’s $4.47 Billion Net Loss, KFF Health News