This is one article I have found which openly supports the 340B program and establishes the reasons for a need of the program. Hospitals located in areas of low income citizens and uninsured patients are more likely to make use of this program than those in more affluent areas. Efforts disparaging this program because of bad players would weigh heavily amongst those institutions located in poorer areas providing care to their clients of need and the uninsured. However . . . Some organizations have closed their hospitals in poorer areas, relocating them to wealthier areas. To qualify for the 340B program, the organization to which the hospital belongs will open up clinical care in the poorer areas so as to qualify. It is expected the discounts are
Topics:
Angry Bear considers the following as important: 340B, Healthcare, Hot Topics, Pharamaceuticals, US EConomics
This could be interesting, too:
NewDealdemocrat writes JOLTS revisions from Yesterday’s Report
Joel Eissenberg writes No Invading Allies Act
Bill Haskell writes The North American Automobile Industry Waits for Trump and the Gov. to Act
Bill Haskell writes Families Struggle Paying for Child Care While Working
This is one article I have found which openly supports the 340B program and establishes the reasons for a need of the program. Hospitals located in areas of low income citizens and uninsured patients are more likely to make use of this program than those in more affluent areas. Efforts disparaging this program because of bad players would weigh heavily amongst those institutions located in poorer areas providing care to their clients of need and the uninsured. However . . .
Some organizations have closed their hospitals in poorer areas, relocating them to wealthier areas. To qualify for the 340B program, the organization to which the hospital belongs will open up clinical care in the poorer areas so as to qualify. It is expected the discounts are also used in the wealthier areas where the hospitals relocate and a higher price for the drugs.
And what if, the hospital does the opposite and maintains the hospital in a needy area. It was found, 26% of off-site clinics in ZIP codes with percent of white residents at least 30% higher than parent hospital in a needy area. And 47% of off-site clinics in ZIP codes with median income at least 30% higher than parent hospital. You begin to understand the issues with the 340B program and the player medical organizations gaming the program.
This does not mean the 340B program should be ended. The IRS and Department of Health and Human Services may be interested in this issue.
Five Reasons for Congress to Protect the 340B Program, RealClearHealth, Laura Boudreau, December 2022
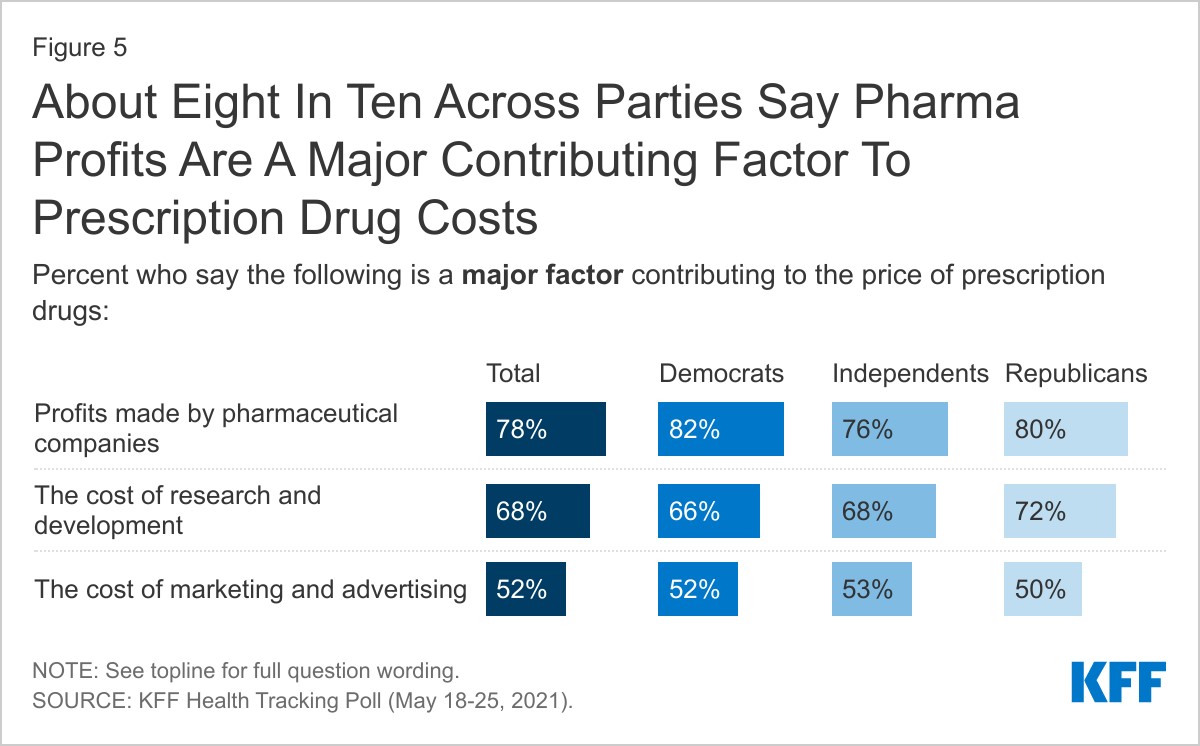
High drug costs are one of the things at the top of the list in anybody’s mind in America. Eight in 10 Americans see drug company profits as a major contributing factor.
No wonder and last year, the U.S. healthcare system spent $776 billion on prescription drugs. The same year, Pfizer’s CEO received over $24 million in annual compensation, not to mention a golden parachute worth nearly $113 million. Meanwhile, millions of Americans have and had to choose between buying groceries, paying rent, or filling their prescriptions.
Drug companies would like nothing better than to change the subject from ever-increasing drug prices and corporate profits and place the blame elsewhere. This a reason they are now targeting the federal 340B Drug Pricing Program and the safety net providers that participate in it. Drug companies recently launched an aggressive attack campaign to vilify the 340B Program and those providers, attempting to destroy or radically scale back the program.
Americans cannot afford this change. The curtain hiding their efforts must be pulled back revealing the drug companies’ true motive which is to increase profits. For decades, the 340B program has successfully lowered drug costs and expanded access to healthcare.
The new Congress should protect the 340B Program. Such can only happen if Americans understand its indispensability to the entire U.S. healthcare system and push back on any effort to change 340B.
Five reasons explaining why 340B is essential to the healthcare safety net:
First, the entities participating in the 340B Program make up America’s healthcare safety net. By creating the 340B Program, Congress’s established goal was to enable public and nonprofit health care providers serving low-income and uninsured patients the ability to purchase drugs at lower costs. These providers are called “covered entities,” and they include federally qualified health centers, children’s disproportionate share hospitals, HIV health centers, and other providers caring for the underserved populations.
Second, the 340B Program costs taxpayers nothing. The federal government effectively grants certain nonprofit and public entities the right to purchase medicine from drug companies at a discount. Think of it as the government giving you (a safety net provider) a discount card, which a drug company must honor when you present the card to buy drugs for your patients.
Third, drug manufacturers want to renege on the deal they struck with the federal government. To be clear:
Drug companies choose to participate in the 340B Program. No one forces them. They participate because, by agreeing to provide discounts to safety net providers, the federal government rewards drug companies with access to the lucrative Medicaid and Medicare markets. Drug companies struck the deal back in 1992. They reaffirmed it in 2010 when the Affordable Care Act expanded Medicaid and added more categories of safety net providers to the list of covered entities. The drug companies are keen on staying in Medicaid and Medicare. They are also keen on ignoring the giving of discounts to safety net providers which was always part of the agreement.
Fourth, drug companies make billions of dollars from the 340B Program. Last year, drug companies made approximately $44 billion in sales to 340B safety net providers. Being realistic, the drug companies profit immensely from the program. By changing or ignoring the specified agreement, they plan to earn more profit by charging full drug prices. This occurring without discounts and without any accountability to ensure their profits are spent for the public good.
Fifth and most important, cutting back or eliminating the 340B Program would cost U.S. taxpayers more and make American patients sicker. The taxpayers’ burden would increase with safety net providers in their communities having fewer resources for services. For example, America’s strategy for ending the HIV epidemic depends on the resources the Ryan White medical providers generate from the 340B Program to provide a host of ancillary services needed to help people living with HIV stay healthy and keep their viral load at undetectable levels. This, in turn, prevents transmission of the virus.
In short, without 340B resources, HIV would become more prevalent in the United States, with more people needing more services and becoming an even heavier burden borne by U.S. taxpayers. That cost is too high. The 340B Program is simply too important, and Congress needs to defend it.